Proximal Convoluted Tubule Reabsorption
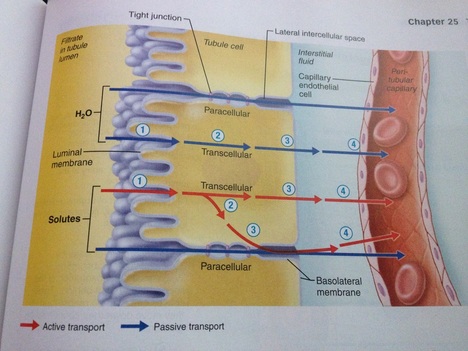
The Proximal convoluted tubule (PCT) is the first part of the nephron where reabsorption of other solutes from the filtrate takes place. This process of selective reabsorption is called tubular reabsorption and solutes from the filtrates are selectively reabsorbed back into the bloodstream, through the surrounding blood capillaries or known to be more specific the peritubular capillaries. The process of tubular reabsorption is a selective transepithelial process that begins as soon as the filtrates enter the PCT. For the reabsorbed substances to reach the blood, the substances follow either the transcellular or paracellular route. If the reabsorbed substance were to take the transcellular route then it would firstly transport the substance across the luminal membrane, diffuse through the cytosol, then have to transport across the basolateral membrane and finally movement through the intestinal fluid surrounding the peritubular capillary and then entering the capillary and back into the bloodstream (refer to the above diagram). Movement of substances in the paracellular route between the tubule cells is limited because these cells are connected by tight junctions. These tight junctions within the PCT area allow some important ions to pass through back into the bloodstream.
Substances such as glucose, amino acids, vitamins, ions such as Na+, K+, Ca2+, Cl-, HCO3-
are actively reabsorbed from the tubule. A prime example are sodium Ions. Sodium ions are the single most abundant in the filtrate, around 80% of energy is used for active transport of sodium back into the bloodstream, making sodium reabsorption always active and via transcellular route. The sodium is actively transported out of the tubule cell by primary active transport via the basolateral Na+ K+ pump. This primary active transport also allows for passive solute diffusion, osmosis and secondary active transport (cotransport) with Na+, allowing nutrients such as glucose, amino acids and vitamins to be reabsorbed back into the blood through secondary active transport.
Instead of active transport there is also passive reabsorption, where urea and water are prime examples of being reabsorbed back into the bloodstream through passive diffusion. Passive tubular reabsorption is the movement of molecules from an area of high concentration to an area of low concentration without the use of energy (ATP). The movement of sodium ions and other solubles back into the bloodstream causes within the PCT a greater osmotic concentration, therefore water moves into the peritubular capillaries by osmosis because there is less concentration of water in the capillaries. As water leaves the tubules within the PCT, the concentration of solutes in the filtrate also increases, and then start to follow the concentration gradients, passively moving these substances in the peritubular capillaries. This can be described as solutes following solvent present in the filtrate and explains the passive reabsorption of a number of solutes present in the filtrate such as urea, moving from a high to low concentration.
Obligatory reabsorption of water is caused by the removal of molecules, this is because in a continuously water permeable environment of the PCT the removal of molecules and ions from the filtrate cause the PCT to be 'obliged' to absorb water regardless of its state whether it be over or under hydration. This water flow is referred to Obligatory water reabsorption, that is essentially caused due to the reabsorption of molecules and ions from the PCT.
The Proximal convoluted tubule (PCT) is the first part of the nephron where reabsorption of other solutes from the filtrate takes place. This process of selective reabsorption is called tubular reabsorption and solutes from the filtrates are selectively reabsorbed back into the bloodstream, through the surrounding blood capillaries or known to be more specific the peritubular capillaries. The process of tubular reabsorption is a selective transepithelial process that begins as soon as the filtrates enter the PCT. For the reabsorbed substances to reach the blood, the substances follow either the transcellular or paracellular route. If the reabsorbed substance were to take the transcellular route then it would firstly transport the substance across the luminal membrane, diffuse through the cytosol, then have to transport across the basolateral membrane and finally movement through the intestinal fluid surrounding the peritubular capillary and then entering the capillary and back into the bloodstream (refer to the above diagram). Movement of substances in the paracellular route between the tubule cells is limited because these cells are connected by tight junctions. These tight junctions within the PCT area allow some important ions to pass through back into the bloodstream.
Substances such as glucose, amino acids, vitamins, ions such as Na+, K+, Ca2+, Cl-, HCO3-
are actively reabsorbed from the tubule. A prime example are sodium Ions. Sodium ions are the single most abundant in the filtrate, around 80% of energy is used for active transport of sodium back into the bloodstream, making sodium reabsorption always active and via transcellular route. The sodium is actively transported out of the tubule cell by primary active transport via the basolateral Na+ K+ pump. This primary active transport also allows for passive solute diffusion, osmosis and secondary active transport (cotransport) with Na+, allowing nutrients such as glucose, amino acids and vitamins to be reabsorbed back into the blood through secondary active transport.
Instead of active transport there is also passive reabsorption, where urea and water are prime examples of being reabsorbed back into the bloodstream through passive diffusion. Passive tubular reabsorption is the movement of molecules from an area of high concentration to an area of low concentration without the use of energy (ATP). The movement of sodium ions and other solubles back into the bloodstream causes within the PCT a greater osmotic concentration, therefore water moves into the peritubular capillaries by osmosis because there is less concentration of water in the capillaries. As water leaves the tubules within the PCT, the concentration of solutes in the filtrate also increases, and then start to follow the concentration gradients, passively moving these substances in the peritubular capillaries. This can be described as solutes following solvent present in the filtrate and explains the passive reabsorption of a number of solutes present in the filtrate such as urea, moving from a high to low concentration.
Obligatory reabsorption of water is caused by the removal of molecules, this is because in a continuously water permeable environment of the PCT the removal of molecules and ions from the filtrate cause the PCT to be 'obliged' to absorb water regardless of its state whether it be over or under hydration. This water flow is referred to Obligatory water reabsorption, that is essentially caused due to the reabsorption of molecules and ions from the PCT.
